

Your brain on (or rather – OFF) oestrogen
This is the kind of day many women with ADHD will recognise:
You wake up tired in a way sleep didn't fix. The coffee or tea doesn't help. Your inbox feels heavier than it did yesterday. The task at the top of your list – a perfectly normal task you've done a hundred times – sits on your screen and you cannot make yourself begin it. You're not depressed. You're not panicking. You're just… stuck. The kind of stuck where every minute that passes makes starting feel slightly more impossible than the minute before.
Most of us have been told this is procrastination. A discipline problem. Something to be fixed by a better morning routine, or a planner, or trying harder.
It isn't. For women with ADHD, this particular flavour of "stuck" often has a specific, predictable, biological driver. And once I understood what was happening, I stopped explaining those days as personal failure, and started planning around them.
The thing nobody told you about oestrogen
When we learn about oestrogen in school, it's filed under "reproduction." Ovaries, menstruation, fertility. A hormone with a clear job, in a clear place.
That picture is incomplete in ways that matter enormously if you have ADHD.
Oestrogen is made in at least four places in the body. Your ovaries are one of them: the primary source during your reproductive years. But oestrogen is also produced in the adrenal glands and fat tissue, which is why it doesn't disappear entirely after menopause as your body quietly keeps making some. And – this is the part almost nobody talks about – it's produced in your brain itself.
Read that again, because it's worth sitting with: your brain is not a passive recipient of oestrogen. It is an oestrogen-producing organ.
Neurons and astrocytes (a type of brain cell that does everything from nourishing neurons to regulating inflammation) synthesise oestradiol locally. They don't wait for oestrogen to arrive from elsewhere. They make their own, right there in the brain tissue, and use it as a neurochemical, to protect brain cells, build synaptic connections, and support memory and learning.
That changes how we need to think about what happens when oestrogen levels shift.
The oestrogen-dopamine dance
Here's where it gets interesting for ADHD specifically.
Oestrogen, from all sources, is one of the most powerful modulators of dopamine. It affects how many dopamine receptors your neurons have, how much dopamine is released, and how efficiently dopamine signalling works in the prefrontal cortex; the very region that's already under-resourced in ADHD brains.
Dopamine is the neurotransmitter your ADHD brain runs short on. It's what makes tasks feel rewarding enough to start. It's what lets you sustain attention on something that isn't intrinsically thrilling.
When oestrogen is high, dopamine signalling works better. Tasks feel doable. Emotions feel regulate-able. Your brain feels, in some hard-to-articulate way, more yours.
When oestrogen drops – whether by a few days in the cycle, or by the months-long shifts of perimenopause – dopamine signalling gets less efficient. And for an ADHD brain that was already operating with less dopamine than average, that drop doesn't just make things a bit harder. It makes things genuinely, measurably worse.
That stuck feeling at your desk? That isn't laziness or lack of discipline. It's a neurochemical reality. The hardware temporarily works less well, because the chemistry modulating the hardware has shifted.
The four windows where this matters most
If you're tracking your own experience alongside this, you'll probably recognise at least one or maybe all four of these windows.
The luteal phase. The week before your period, when oestrogen drops. Many ADHD women describe this week as the "my brain is off" week. Tasks that felt easy two weeks ago feel impossible. Emotions are bigger. Sleep is worse. Rejection sensitivity spikes. Recent research confirms what many women have always known: ADHD symptoms, and the effectiveness of ADHD medication, vary measurably across the menstrual cycle, with worsening in the mid-luteal and pre-menstrual phases.
Postpartum. Oestrogen doesn't gently decline after birth – it crashes. Dramatically. ADHD women are significantly more likely to experience severe postpartum depression, cognitive fog, and what many describe as "I don't recognise myself anymore." This is not a character failure. This is a neurochemistry event.
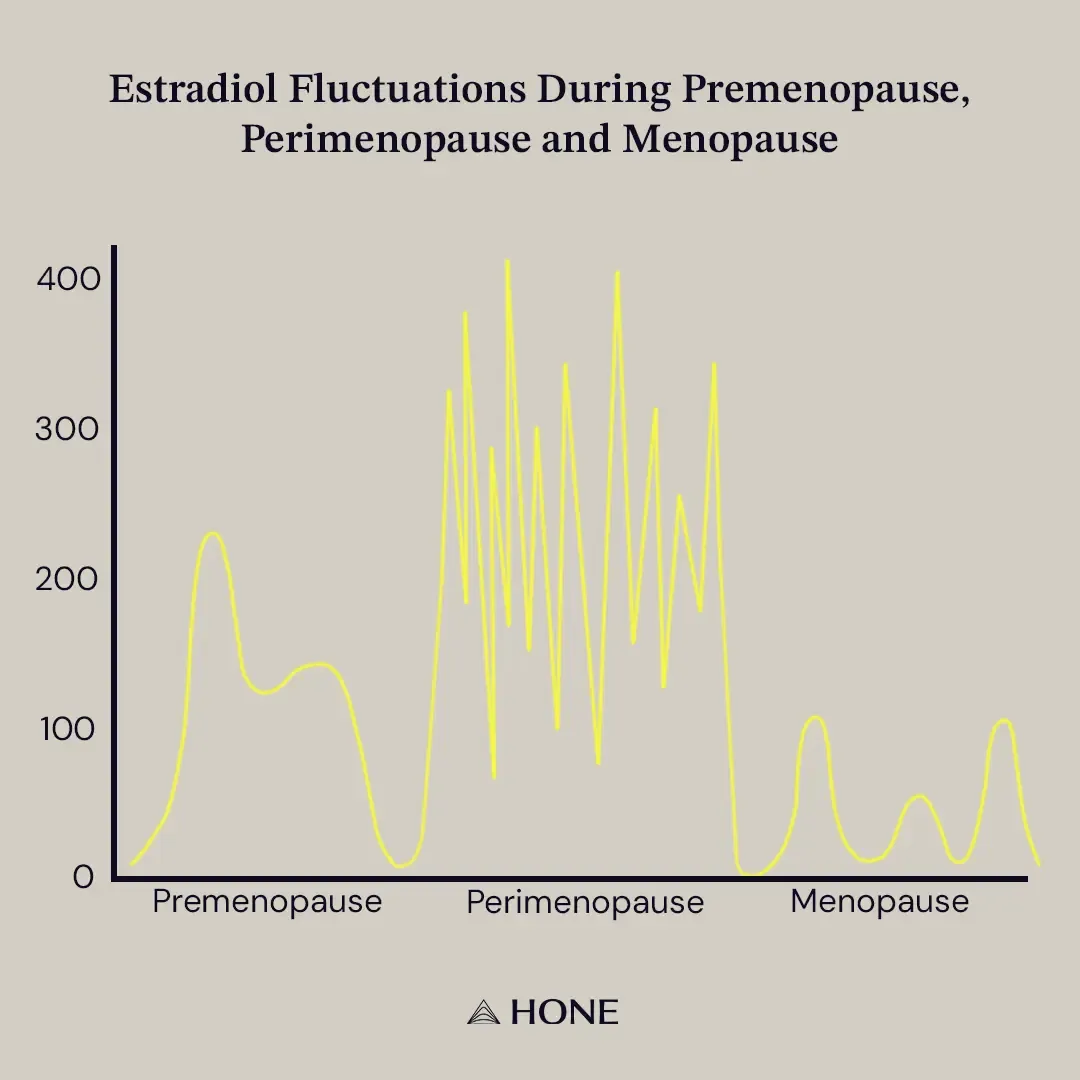
Perimenopause. Oestrogen doesn't drop linearly – it fluctuates wildly, often for 8-10 years before menopause actually arrives. This is why so many women in their late 30s and 40s report a sudden deterioration in functioning that doesn't fit any of the usual explanations. Symptoms you've managed for decades suddenly feel unmanageable. Medications that worked stop working. The coping structures that held up your career start to wobble.
Menopause and beyond. Oestrogen stabilises at a lower level. For some women, symptoms actually improve at this stage because the fluctuation stops. For others, the lower baseline is its own challenge.
What to do with this information
I want to be clear: I am a coach, not a clinician. What follows is not medical advice. It's the set of questions and conversations I'd want every ADHD woman to be having with her own GP, menopause specialist, and (if applicable) ADHD-prescribing psychiatrist.
Track your cycle against your cognition, not just your mood. Note the days your focus goes. The days your rejection sensitivity spikes. The days a two-paragraph email feels insurmountable. Most women are astonished by how patterned their "bad days" turn out to be. Patterns are planning opportunities. This is increasingly being recommended in clinical literature too.
Ask about medication adjustment across the cycle. For women on ADHD medication, fixed doses that work at day 10 often don't work at day 25. This is an emerging clinical conversation: early evidence suggests psychostimulant efficacy varies measurably across the cycle, and some specialists now consider cyclic dosing or supplementary strategies for the luteal week.
Ask about HRT – but read the next section if you've had breast cancer. The research on HRT and ADHD symptoms is still developing, but early evidence is promising, and clinicians who specialise in ADHD and perimenopause are increasingly including it in the conversation. If your GP says "you're too young for that," it's worth knowing that emerging research suggests perimenopause may begin substantially earlier in women with ADHD. A 2025 population study of over 5,000 women found that ADHD-related perimenopausal symptoms peaked at ages 35–39, compared with 45–49 in women without ADHD, suggesting onset up to a decade earlier. So if you're being told you're too young, you may not be, and a referral to a menopause specialist familiar with ADHD is a reasonable next step.
Plan around your brain, not against it. The single biggest shift my clients make is not fighting the dip. The luteal week isn't a week to launch a new project or have a difficult boundary conversation. It's a week for admin, routine work, and being gentle with yourself. Working with your neurochemistry is not defeat. It's self-respect.
A note for breast cancer survivors
I want to flag something my own background makes me particularly aware of, because I spent my doctorate researching oestrogen-driven breast cancer.
Around 70-80% of breast cancers are oestrogen receptor-positive, meaning they can be stimulated to grow by oestrogen. For women who have had this type of breast cancer, systemic HRT has historically been considered contraindicated, and is currently recommended in the UK only in "exceptional circumstances." That's not a wall you've imagined. It's a real, evidence-based caution.
The conversation is genuinely shifting, though. A 2025 expert consensus published in Menopause is calling for a more patient-centred, individualised approach, recognising that for some women with lower-risk cancers and severe menopausal symptoms, the trade-off may look different than a blanket prohibition allows. Vaginal oestrogen, in particular, is now considered low-risk for recurrence due to minimal systemic absorption.
If this is your situation, the questions worth bringing to your medical team are: What was the receptor status of my cancer? What's my current recurrence risk? Are there forms of hormonal support I could safely consider? And separately, what non-hormonal options exist that might help with cognitive symptoms specifically?
You should be involved in this conversation. Not excluded from it.
One final thought
The women I coach didn't learn any of this in school, at work, or from the first GP they mentioned it to. Most of them figured it out in their forties, after a decade of being told they were anxious, hormonal, dramatic or "just burnt out."
We deserved to know this earlier.
And if you've read this far and recognised yourself in it – that recognition is the reason I write this newsletter.
Until next Wednesday!
Warmly,

Did this resonate with you?
Book a free 30-minute clarity call. No pitch, no pressure – just a calm, supportive conversation about where you are right now and whether working together would be a good fit.
PREVIOUS ISSUES
Subscribe to my weekly newsletter "The Dopamine Draft" & other updates below
Subscribe to my weekly newsletter "The Dopamine Draft" and other updates below


© 2026 Reframed & Focused Coaching
© 2026 Reframed & Focused Coaching